How maths can help us fight infectious diseases

Epidemics make interesting news stories. Dramatic headlines are often accompanied by pictures of healthcare workers in full-body protective equipment or laboratory researchers at microscopes. What does not often feature, however, are pictures of the mathematicians working behind the scenes to understand and predict how infections spread.
Mathematical models are used to create a simplified representation of infection spread in a population and to understand how an infection may progress in the future. These predictions can help us to use public health resources such as hospital space or a vaccination programme more effectively. For example, knowing how many people in a population are likely to become infected can tell hospitals how much space and resources they will need to allocate for treatment.
Making a mathematical model of a disease starts with some basic principles that are similar whether you are looking at Ebola or E. coli, the human population or populations of cells in the body. Most simply, models classify people into states based on their infection status. For example, if nine people in a population of ten are not infected by a particular pathogen they are “susceptible” [S]. The remaining person who has the infection and can pass it on to others is “infectious” [I]. Anyone who had the infection and survives to become resistant to it is “immune” [R].
The diagram below shows the basic structure of this “SIR” model, the most commonly applied mathematical model for pathogens such a chicken pox. Other pathogens may require slightly different models. For example, pathogens that can be caught again such as gonorrhoea will often not include an immune stage. Some pathogens such as Ebola include an “exposed” stage where the individual is infected but is not yet capable of passing on the infection.

Simple SIR model
Author provided
A model is made unique to a particular scenario with information about the population being studied and the infecting pathogen. This can include how contagious a pathogen is, how long an individual remains infectious for, the population size, and the number of infectious people at a given time.
Models can also include information about how different parts of the population – such as adults and children, men and women – interact and how the pathogen is spread, for example through sneezing or sexual contact. Whether an individual has previously been infected or vaccinated can also alter the model, with these individuals initially classified as immune and not susceptible. This is something that is incorporated in to a measles model, as many individuals are vaccinated against this virus in childhood.
This information on the population and the pathogen is used to create equations that calculate how quickly people move between the different states. Using our above example, we can calculate the rate at which susceptible people become infectious, expressed as “b”. This is dictated by the total population size (10) and the chance that the pathogen will be passed between two people, let’s say 80%.
The transmission rate per person would then be 80% (or 0.8) divided by 10, or 0.08. If we then multiply this by the number of people already infectious (1) and those who are susceptible (9) we get 0.08 x 9 x 1 = 0.72. That means that, on average, just under one person becomes infected per day.
Once a model is set-up, it is then run forward in time to project how the infection will progress. The model output in the graph below shows a population of 100 people starting with 99 susceptible, one infectious and no immune individuals. As time advances, the number of individuals in each state changes as susceptible people become infectious then are replaced by those who become immune. By day seven, the infection has died out, leaving 60% of the population immune following infection and 40% still susceptible.
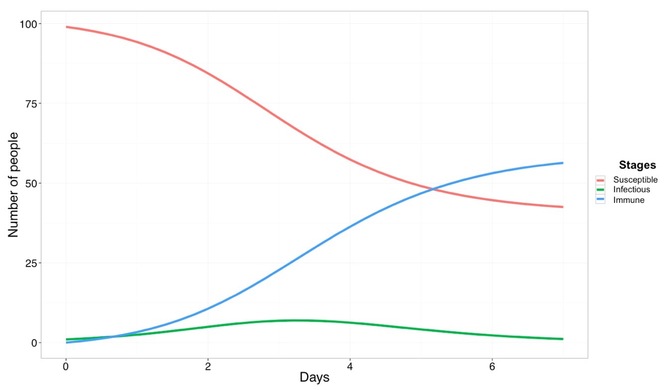
Model over time
Author provided
To determine if the model is a true representation of infection in a population, we can match its results to recent or current infection data. The more closely the model output matches the real data, the more likely it is that the model represents the true situation. Once a model fits known infection data, we can assume it will predict future infection trends reasonably well (if other circumstances do not change).
When it comes to real-world application, mathematical models have had a direct impact on best practices in public health. For example, modelling was used to determine whether new vaccines for tuberculosis (TB) would have a greater impact on lowering disease prevalence if given to children or adults.
The study found that more cases of TB could be prevented before 2050 at a lower cost if any new vaccines developed for the disease were given to adults. On the basis of these findings, along with additional evidence, clinical trials for new TB vaccines are now being designed to recruit adults as a target population to vaccinate.
In our globally connected world, pathogens will continue to emerge or re-emerge and spread. Models allow us to make powerful predictions about future infections using information from the present. This allows mathematical modellers to provide essential recommendations to the health care workers that we see wearing full-body protective equipment, contributing to reducing the spread of infection and improving global health.![]()
This article is published in collaboration with The Conversation. Publication does not imply endorsement of views by the World Economic Forum.
To keep up with Agenda subscribe to our weekly newsletter.
Author: Erin Lafferty is Research fellow at London School of Hygiene & Tropical Medicine and Gwen Knight is Research fellow at London School of Hygiene & Tropical Medicine
Image: A health inspection and quarantine researcher demonstrates to customs policemen the symptoms of Ebola, at a laboratory at an airport in Qingdao, Shandong province. REUTERS/China Daily
Don't miss any update on this topic
Create a free account and access your personalized content collection with our latest publications and analyses.
License and Republishing
World Economic Forum articles may be republished in accordance with the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International Public License, and in accordance with our Terms of Use.
The views expressed in this article are those of the author alone and not the World Economic Forum.
Stay up to date:
Digital Communications
Related topics:

Forum Stories newsletter
Bringing you weekly curated insights and analysis on the global issues that matter.
More on Emerging TechnologiesSee all

Dr Gideon Lapidoth and Madeleine North
November 17, 2025




