Why quality data is key to healthcare AI fulfilling its promise

AI-driven models of healthcare can improve diagnostics by unifying data. Image: Getty Images/Unsplash
- Healthcare systems worldwide are fragmented as records don't travel with patients and data stops at institutional borders.
- AI-driven healthcare models can address this issue but are hindered by a shortfall in the underlying architecture on which they run.
- Abu Dhabi’s Intelligent Health System offers a working blueprint for others by treating health intelligence as a foundational service rather than an application layer.
A 58-year-old diabetic patient sees her primary care physician at one healthcare provider, her endocrinologist at another, and then collects her medication from two pharmacies near her home.
Each health system holds only a fragment of her story. When she arrives at the hospital emergency room with new onset chest pain, the physician sees a record that appears complete but is actually missing the medication interaction that would have flagged her risk three days earlier.
The AI model that would have caught this has existed for years. The shortfall is not one of intelligence, but infrastructure.
This patient’s experience is not an anomaly. Across every continent, health systems face the same structural failure: records that don't travel with patients, data that stops at institutional borders, and artificial intelligence (AI) models running on foundations that were never built for them. The technology has advanced, but the underlying architecture has not.
Health data fragmented across systems
Her data, like the data of billions of patients worldwide, is scattered across systems that were never designed to share it. Electronic health records don’t interoperate. Pharmacy databases live in isolation. Insurance systems optimize for billing, not insights. The substrate on which healthcare AI must run was never built for this crucible moment.
This is the challenge we do not discuss enough: healthcare AI is not held back by inadequate models, but by a missing layer, the invisible architecture that enables those models to actually work.
When healthcare leaders talk about interoperability, it is often framed as a technical problem, when it is, in fact, a governance challenge.
Organizations making real progress on production-grade AI recognize this. They see intelligent data as an organizational brain and elevate data unification to an executive priority. They assign accountability to clinical, operational and tech leaders.
Regulatory frameworks have laid much of the groundwork. EU interoperability mandates, Fast Healthcare Interoperability (FHIR) adoption in the US, India's Ayushman Bharat Digital Mission, and the World Health Organization's Global Strategy on Digital Health all point in the same direction. What is consistently missing is institutional will – the decision to treat data unification as strategic infrastructure rather than a compliance checkbox.
The organizations stuck in perpetual pilot phases share common patterns: they invest in sophisticated AI tools while leaving their data foundations fragmented. McKinsey research points to fewer than 20% of healthcare AI pilots successfully transitioning to full-scale deployment, and Massachusetts Institute of Technology’s (MIT) 2025 study found that 95% of AI experiments do not deliver value.
The visibility gap of healthcare data
In consumer AI, approximation often suffices. A recommendation engine that is 80% accurate still delivers value to the user, and even if it misses context, it can be corrected with a second query.
However, healthcare AI operates under different constraints. Missed medication interactions are not a minor inconvenience, diagnostic suggestions based on incomplete history are not merely suboptimal. In healthcare, the margin between “good enough” and “actually sufficient” is measured in patient outcomes.
This reality demands a higher standard of data quality than most health systems, payers and regulators currently achieve. Production-grade healthcare AI requires longitudinal records that capture a patient’s full history, not just their encounters within a single system.
It also requires contextual data such as social determinants that traditional medical records were never designed to hold. Systems are still far from this standard, and no amount of model sophistication can compensate for data that is incomplete at its source.
Patients are starting to notice. The widespread adoption of consumer technology has trained people to expect AI that works.
More than 900 million people worldwide interact weekly with AI assistants like ChatGPT, systems trained to anticipate their needs, surface relevant information, and work across every device they own. Then they walk into a healthcare setting, they encounter fax machines, redundant intake forms and clinicians who cannot access records from a hospital across town.
This gap in experience is a source of institutional pressure. Patients increasingly expect their health systems to demonstrate the same intelligence they encounter elsewhere in their lives.
3 ways to bridge the healthcare data gap
The missing layer is buildable, and it does not require replacing existing systems wholesale. What it does require is a structurally different approach to data architecture, one that unifies information without demanding that every legacy system be ripped out and rebuilt. Three capabilities define this approach.
First, data unification that sits above existing systems, drawing from electronic medical records, pharmacy platforms, claims databases and ancillary sources without requiring each to be replaced.
Second, multimodal normalization that ingests real data in the messy formats it actually arrives in – faxes, unstructured clinical notes, call transcripts – and transforms it into structured, query-able form.
Third, intelligent ontologies and knowledge graphs that turn static data storage into reasoning-ready assets, effectively an infrastructure that holds information and understands its relationships. Two decisions can unlock this: providers designating data infrastructure as a priority and payers redefining quality metrics to reward longitudinal data coverage, not just point-of-care documentation.
Abu Dhabi offers blueprint for intelligent health
This is not a vision for some distant future, Abu Dhabi’s Intelligent Health System offers a working blueprint, as outlined in the World Economic Forum white paper A New Era for Digital Health: Abu Dhabi’s Leap to Health Intelligence.
By treating health intelligence as a foundational service rather than an application layer, the emirate has moved from fragmented digitization to AI-enabled, population-scale care coordination.
In practice, the Abu Dhabi system integrates data across more than 50 health entities, enabling real-time clinical decision support and population-level risk stratification.
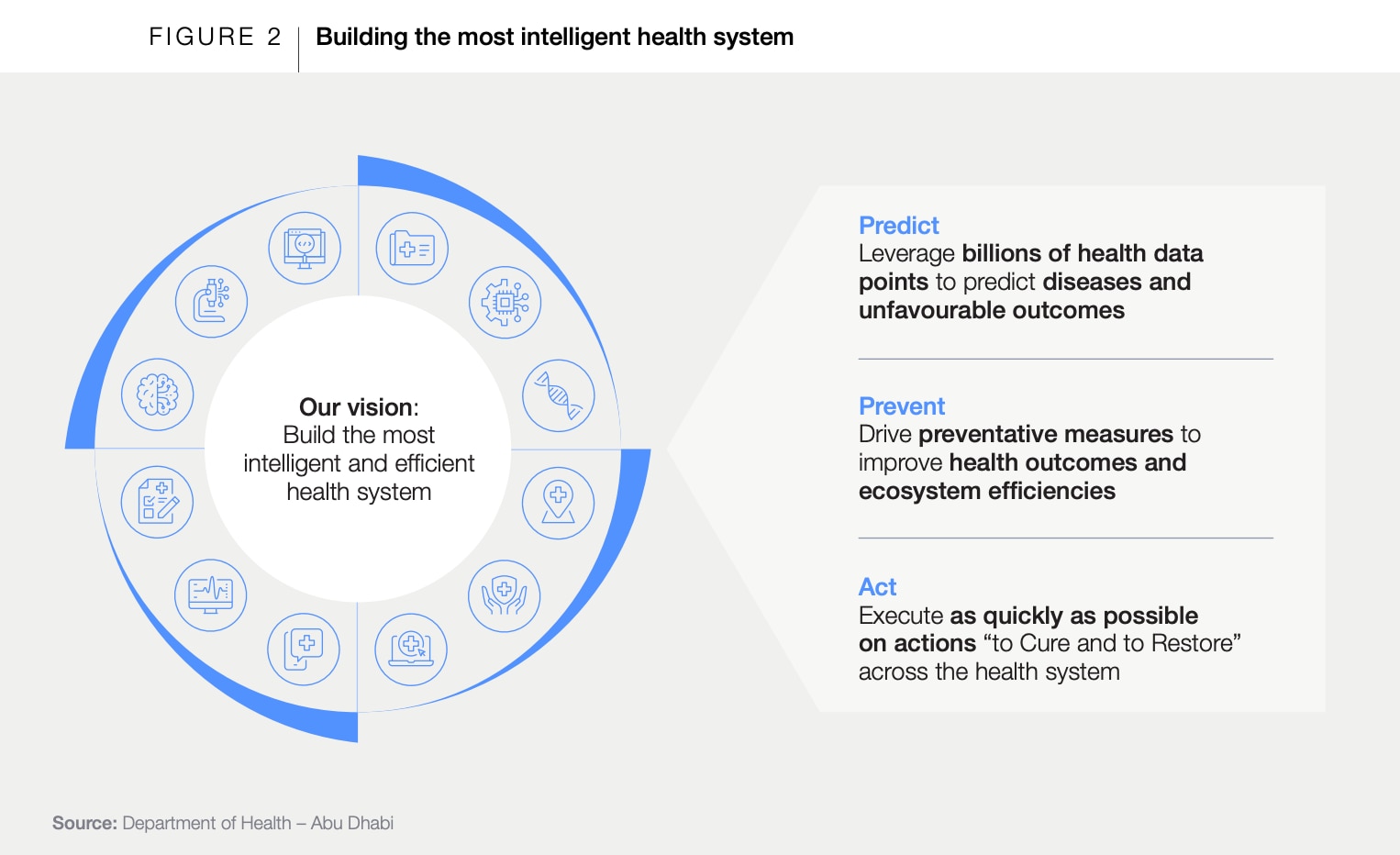
Physicians can access a patient's records across public and private facilities, a function that, in most health systems, requires manual coordination across weeks. The result is measurable: reduced duplication of diagnostics, earlier intervention in chronic disease management and a governance model other health authorities can replicate.
In this way, Abu Dhabi’s Intelligent Health System helps improve health outcomes and ecosystem efficiencies, and serves as an example for others to follow as they recognize healthcare AI as the priority it must become.
How healthcare AI can reimagine the patient’s story
Let’s return to that 58-year-old patient arriving at the emergency room.
In our reimagined version, the system already knows her healthcare issues, her records have been unified across points of care, and the medication interaction has been flagged before she arrives.
The attending physician sees a complete picture, not fragments. The intervention happens in the moments it matters, not days late. On the same day, she is healthy and back home, with no risky admission to hospital and no unnecessary medical expenses.
This future is not a fantasy. The models exist and the standards exist. What remains is the commitment to build the foundational layer that connects them. This commitment must be developed by providers, enabled by payers, and guided by regulators; no single actor can achieve it alone.
The most critical infrastructure is often the part no one notices, the silent architecture that allows everything else to function.
When it comes to healthcare AI, that architecture is still missing. Building it is the work that remains, because technology is most visible when it breaks and at its best when it is invisible.
Don't miss any update on this topic
Create a free account and access your personalized content collection with our latest publications and analyses.
License and Republishing
World Economic Forum articles may be republished in accordance with the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International Public License, and in accordance with our Terms of Use.
The views expressed in this article are those of the author alone and not the World Economic Forum.
Stay up to date:
Data Policy
Related topics:

Forum Stories newsletter
Bringing you weekly curated insights and analysis on the global issues that matter.
More on Health and Healthcare SystemsSee all

Geoffrey Clapp
July 2, 2026





